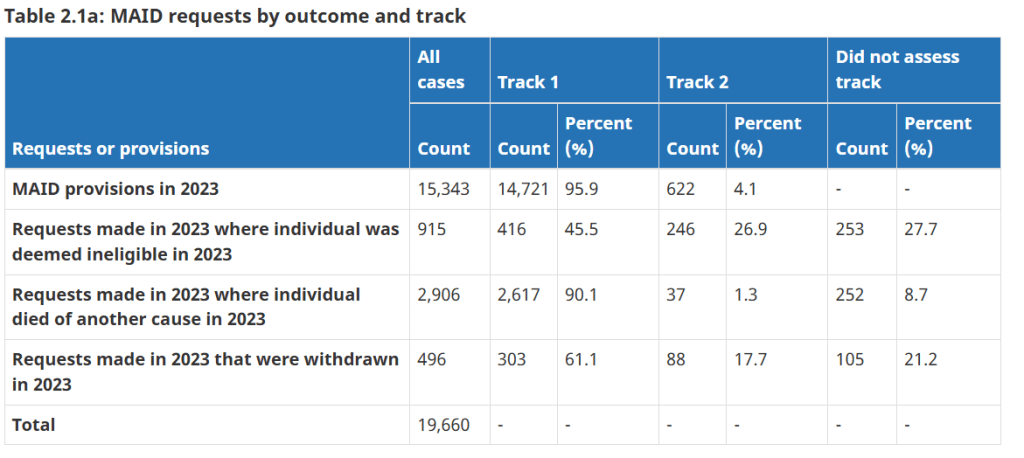
Health Canada released its fifth annual report on medical assistance in dying (MAiD) on December 11, 2024. The report “provides a summary of MAID requests, assessments and provisions for the 2023 calendar year.” To view a PDF version of he report, click the image of he cover below.
The December 2024 report is the first report to present data collected under the amended Regulations for the Monitoring of Medical Assistance in Dying, which came into force on January 1, 2023. The data includes new information on who requested MAiD, what health and other support services were offered and, where possible, how assessments were informed. Given that this was the first year collecting these additional variables, including self-identification measures such as race, Indigenous identity, and disability, there are some important data limitations to consider, including: an inability to present trends over time, some missing data, and limited quality and reliability of some measures. Nevertheless, the report provides important insight into who requested and received MAID, as well as how and where it was delivered.
TVO’s The Agenda hosted a discussion of the report early in 2025.
Humanists Should Analyze and Discuss this Issue
If you’re interested in analyzing and discussing this issue, there are actions you can take. First, here at Humanist Heritage Canada (Humanist Freedoms), we are open to receiving your well-written articles regarding MAiD.
A federal election is likely to be held in Canada in 2025. MAiD will likely be a significant “hot button” issue in the election as politicians seek out issues that will attract voters. Canadian humanists who value their rights and freedoms can help to ensure discussions of MAiD are based on fact rather than emotion and rhetoric. Is there a better place to start than within humanist publications and communities?
What do Canada’s Humanist Organizations have to say about this contemporary human rights matter?
BC Humanists: Medical assistance in dying should be available for any Canadian who freely chooses it, even if they are not terminally ill. There is no moral argument to limit access to a physician-assisted death to individuals with “a grievous and irremediable medical condition.” Safeguards should ensure that decisions are free, voluntary, and informed but should not make access unjustly difficult. Medical assistance in dying should be guaranteed through the publicly funded healthcare system and institutions that refuse should see their funding removed. Ian Bushfield, BC Humanists’ Executive Director told us that, “it’s reasonable to say we support the expansion of MAID to persons whose sole underlying condition is a mental illness.“
Continued or increased restrictions to accessing MAID do not serve to protect the disabled but rather perpetuate a paternalistic relationship between the government and those individuals. To ensure the equal dignity of all people, we must afford everyone choice in life and choice in death.
By continuing to access, link to, or use this website and/or podcast, you accept the HumanistFreedoms.com and HumanistHeritageCanada.ca Terms of Service in full. If you disagree with the terms of service in whole or in part, you must not use the website, podcast or other material.
The views, opinions and analyses expressed in the articles on Humanist Freedoms are those of the contributor(s) and do not necessarily reflect the views or opinions of the publishers.
The Ultimate Choice, a groundbreaking docuseries from TVO Today, with the Toronto Star and the Investigative Journalism Bureau was released on January 25, 2024. It follows the journey of Michael and his wife, Ann. Michael, housebound by pain and incurable disease, sees his choice for a medically assisted death (MAiD) as a powerful solution to his suffering. The series explores Michael’s motivations and how his decision affects his family, friends, and longtime doctor. Hosted by investigative reporter Rob Cribb, the podcast also challenges him to come to terms with his own family history as he dives into this highly charged story. Both a portrait of a family’s autonomy and a hard-hitting exposé, The Ultimate Choice reveals the political and ethical stakes behind Canada’s debate to expand MAID like never before.
What do Canada’s Humanist Organizations have to say about this contemporary human rights matter?
BC Humanists: Medical assistance in dying should be available for any Canadian who freely chooses it, even if they are not terminally ill. There is no moral argument to limit access to a physician-assisted death to individuals with “a grievous and irremediable medical condition.” Safeguards should ensure that decisions are free, voluntary, and informed but should not make access unjustly difficult. Medical assistance in dying should be guaranteed through the publicly funded healthcare system and institutions that refuse should see their funding removed. Ian Bushfield, BC Humanists’ Executive Director told us that, “it’s reasonable to say we support the expansion of MAID to persons whose sole underlying condition is a mental illness.“
Continued or increased restrictions to accessing MAID do not serve to protect the disabled but rather perpetuate a paternalistic relationship between the government and those individuals. To ensure the equal dignity of all people, we must afford everyone choice in life and choice in death.
By continuing to access, link to, or use this website and/or podcast, you accept the HumanistFreedoms.com and HumanistHeritageCanada.ca Terms of Service in full. If you disagree with the terms of service in whole or in part, you must not use the website, podcast or other material.
The views, opinions and analyses expressed in the articles on Humanist Freedoms are those of the contributor(s) and do not necessarily reflect the views or opinions of the publishers.
According to their website, The Canadian Hospice Palliative Care Association (CHPCA) is “the national voice forHospice Palliative Care in Canada. Advancing and advocating for quality end-of-life/hospice palliative care in Canada, its work includes public policy, public education and awareness. Established in 1991, its volunteer Board of Directors is composed of hospice palliative care workers and volunteers from Canadian provinces and territories as well as members-at-large.”
It is always interesting to observe an organization declare itself to be “the” national voice for this, that or the other thing. That particular phrasing seems to presume, preclude or presuppose a variety of details, matters and alternatives. While this article isn’t an exploration of how organizations may be created out of nothing more than a handful of individuals with a common interest to become The National Voice on a given topic, it is interesting to note that the Government of Canada says that applying to be a charity is a four-step process. You’d think it would be more complicated than that.
On a rather tangential detail, did you know that Sue Rodriguez was diagnosed with amyotrophic lateral sclerosis (ALS) — also known as Lou Gehrig’s disease — a quickly progressing neurological disease that attacks the nerve cells controlling voluntary muscle movement in 1991?
At that time, medical assistance in dying was illegal in Canada.
While the timeline of CHPCA’s creation and Sue Rodriguez’s diagnosis may earnestly be assumed as nothing more than coincidence, it does make one wonder what CHPCA’s policies and attitudes may be about medical assistance in dying. Fortunately, CHPCA has a page on their website dedicated to ethics. On that page, it says:
Palliative Sedation
Palliative sedation refers to the use of pharmacological agents to reduce consciousness with the intention of providing relief for intractable symptoms when all other possible therapeutic options have failed. This intervention is only considered in a patient who has been diagnosed with an advanced progressive illness and typically the patient is perceived to be close to death (i.e. in the last two weeks of life). Generally, the goal is the lowest level of sedation required to achieve the desired comfort level/control of symptoms; therefore, specific pharmacological agents are generally started at the smallest possible dose and titrated upwards to effect. This therapy is distinct from medical assistance in dying, as the intention is not to hasten death or shorten one’s life. Common indications include intractable cases of agitated delirium or dyspnea, massive hemorrhaging, and refractory seizures—all of which are extremely distressing to a patient3. The role of palliative sedation in psychological, spiritual, or existential distress is unclear. Commonly, the experience of having a patient sedated can be a conflicting and emotional time for families and caregivers; it is therefore crucial to ensure they receive appropriate psychosocial and spiritual support.
Responding to requests for assisted dying
When patients are confronted by their life-limiting illness and experience loss of function in their day-to-day lives due to their disease, it can be very distressing. In their suffering, some patients become compelled to wish for a hastened death. Some of those patients may endorse some passive suicidal thoughts, whereas others are insistent about wanting to end their lives in a specific moment with medical assistance. With recent developments in the movement for medical assistance in dying (MAID) in Canada, it is important for healthcare practitioners to recognize these requests and respond appropriately. Regardless of whether an individual healthcare practitioner supports or stands against this controversial topic, it is important that patients are still heard. Perhaps patients fear a protracted disease course with intractable symptoms, or they are distressed by the disability that their illness brings—regardless of what is driving their request, it is crucial for healthcare practitioners to recognize that there is some unaddressed suffering at the root of this request that needs further exploration.
On another tangential note. It wasn’t our idea to place those two paragraphs together. That’s the way we found them. The bold font is, admittedly, our innovation.
Despite CHPCA’s suggestion that palliative sedation’s role in distress is unclear, it does seem clear that CHPCA’s ethics suggest that dosing someone into un- or semi-consciousness in the clinically-expected final two weeks of their existence is reasonable as well as clinically and ethically sound.It may also be observed that CHPCA understands that patients should be heard. One wonders how articulate an individual who has been medicated into un- or semi-consciousness may be.
For those who are able to communicate strongly enough that their care-takers hear them, CHPCA’s ethics also make clear that any unaddressed suffering still needs to be explored. Even during the clinically-expected final two weeks of life. Ethics is such an interesting term.
While still able to make her voice heard, Sue Rodriguez asked whose life it was to continue or end, if not her own. It would be interesting and informative if CHPCA posted a clear, direct and unequivocal answer to that question on their ethics website.
Until then we’ll just have to infer.
On an Unrelated Matter
Dying With Dignity Canada (DWDC) is the national human-rights charity committed to improving quality of dying, protecting end-of-life rights, and helping people across Canada avoid unwanted suffering.
DWDC hosted the 2022 World Federation of Right to Die Societies (WFRTDS) International Conference in Toronto from November 3 to 6, 2022. The event brought international delegates and local attendees together. It was the must-attend event for clinicians, lawyers, advocates, and supporters who wanted to learn more about assisted dying in Canada and around the world.
DWDC’s 2023 to 2025 strategic plan states that the organization will “lead national advocacy efforts to eliminate obstacles to end-of-life choice, including access to advance requests and end forced transfers.” This is in an effort to:
To protect the constitutional right of Canadians to MAID
To identify and remove new and ongoing barriers and challenges to choice-in-dying
To ensure accurate information is easily available
What is a “forced transfer“? It seems to be what may happen if you’d rather end any unaddressed suffering in the final days of your life rather than be medicated into unconsciousness or have your suffering otherwise explored.
HumanistFreedoms.com wonders how long it will be until some ethical folks take the necessary four steps to ensure that there are institutions and facilities in place that provide a straight-forward palliative care alternative to all this forced transfer bullshit. But we suppose that things are probably more complicated than that.
The views, opinions and analyses expressed in the articles on Humanist Freedoms are those of the contributor(s) and do not necessarily reflect the views or opinions of the publishers.