You may wish to read Critically Thinking About COVID19 PART I, Critically Thinking About COVID19 PART II and Critically Thinking About COVID19 PART III before diving into this essay.
By: Dr. Christopher DiCarlo (December 18 , 2020)
In this installment of commentary on the current Covid19 pandemic, we will consider our current status in regards to testing, restrictions, vaccination development, and public policies. As usual, in light of our epistemic model, it is always important to remember Rumsfeld’s Rule:
“There are known knowns. There are things we know that we know. There are known unknowns. That is to say, there are things that we now know we don’t know. But there are also unknown unknowns. There are things we do not know we don’t know.”[1]
So at this point in the pandemic, we must ask ourselves: what do we know, and what do we know we don’t know about this particular virus?
Controlling the Spread of the Disease:
It is important to understand that there are three ontological states of being when it comes to human infection: asymptomatic, pre-symptomatic, and symptomatic. We have known for quite some time that many spreaders of the disease have been asymptomatic i.e. those infected but who exhibit no symptoms. Because of various studies carried out by different countries around the world – including Iceland, the UK, and others, we are starting to see a clearer picture on the actual percentage of asymptomatic carriers of the virus.[2] Coming in somewhere between 75% and 86%, we are discovering that one of the central reasons such a virus can spread so quickly is not simply due to its high level of virulence i.e. ability to infect a host, but to the fact that so many people don’t even realize they have it, and therefore, don’t self-isolate.

At this point in the pandemic, we are starting to see some variance in regards to viral mutations throughout the world. The UK has found that several new mutations have arisen, some of which have made the virus more communicable, others making the virus somewhat weaker:
The new strain of coronavirus spreading through Britain has a ‘striking’ amount of mutations, scientists have claimed. Members of the UK’s Covid-19 Genomics UK Consortium (COG-UK), who have been investigating the evolved strain, say they have uncovered 17 alterations, which they described as ‘a lot’. Many of the changes have occurred on the virus’s spike protein, which it uses to latch onto human cells and cause illness. Alterations to the spike are significant because most Covid vaccines in the works, including Pfizer/BioNTech’s approved jab, work by targeting this protein.[3]
These mutations have some people worried that the currently developed vaccines will not have any effect on these variants. “But scientists, including England’s chief medical officer Chris Whitty, have said there is ‘currently no evidence’ the mutation — which has been spotted in Wales, Scotland, Denmark and Australia — will have any impact on vaccines.”[4] So that is some good news as we face this second and far more devastating wave of infections. But we must also remember, that such a virus will continue to evolve and mutate even after massive vaccinations have been carried out:
…vaccines won’t put an end to the evolution of this coronavirus, as David A. Kennedy and Andrew F. Read of The Pennsylvania State University, specialists in viral resistance to vaccines, wrote in PLoS Biology recently. Instead, they could even drive new evolutionary change. There is always the chance, though small, the authors write, that the virus could evolve resistance to a vaccine, what researchers call “viral escape.” They urge monitoring of vaccine effects and viral response, just in case.[5]
A lot of people don’t realize this, but there will be scientists who will track the mutation rates of Covid-19 for months or even years after global inoculations have taken place. We can be fairly optimistic that with the various vaccines in circulation now, the likelihood for ineffectiveness over time remains fairly low:
There are some reasons to be optimistic that the coronavirus will not become resistant to vaccines. Several years ago, Dr. Kennedy and Dr. Read presented an analysis of the difference between resistance to drugs and vaccines. Neither bacteria nor viruses evolve resistance to vaccines as easily as they do to drugs, they wrote. Smallpox vaccine never lost its effectiveness, nor did the vaccines for measles or polio, despite years of use.[6]
So it looks as though we can rest assured that scientists will not have to continuously battle an ever-changing, shape-shifting, virus in the years to come.
And let’s remember, a global viral pandemic will always follow this exact pattern of reaction: Testing, Isolation, Anti-virals, and Vaccine (or TIAV)
To return to our acronym – TIAV, let’s where we’re at in terms of current information:
Testing: “Don’t let the perfect be the enemy of the possible”
In regards to testing, there have been some developments since my last paper in September but quite frankly, I’m disappointed in the overall failure of testing placement by our local, provincial, and federal governments. Where are the ‘at-home self-tests’ for Covid-19? They exist, but they have not been approved for wide distribution and use. In my last paper, I had discovered that Precision Biomonitoring received approval for their PCR rapid testing units on July 7th. But neither the Provincial nor Federal Governments purchased any such devices. Instead, major Canadian and US companies purchased them which allowed mining, fishing, logging, and even the movie industries to continue with little interruptions. Had our governments purchased such units and hired the right people to put them in key places such as airports, retirement homes, supply chains, private businesses, etc., we could have minimized the effects of the inevitable second wave of infections. Be that as it may, we are still using the same, basic testing facilities that have been in place since March, 2020. The response times are still anywhere from 2-5 days which is helpful but still far too long to have any significant impact on controlling and tracing the spread of the virus.
What I referred to in earlier papers as the ‘Holy Grail’ of tests, may finally be a reality. The FDA just recently announced its Emergency Use Approval for the first fully at-home Covid-19 Test by Ellume.[7] Although not as accurate as the PCR tests, medical authorities believe they will go a long way in allowing people to safely test themselves from the comfort of their own home rather than having to wait in line ups and wait for days for results.
In terms of accuracy,
With all antigen tests, positive results are highly accurate and should be treated as a presumptive positive (meaning, you should act as though you have Covid until another test can verify it). However, there is a higher chance of false negatives, because antigen levels can drop lower than what the tests can detect, according to the FDA. In other words, a negative antigen test result doesn’t rule out a Covid-19 infection. Clinical trials found that Ellume’s home test correctly identified 96% of positive samples and 100% of negative samples in people with Covid symptoms. In people without symptoms, the test correctly identified 91% of positive samples and 96% of negative samples. That means this test works best with people who have Covid symptoms, because antigen tests return positive test results when a person is most infectious. So, while this test can save you a trip to a clinic and a long wait in line to get antigen tested, the results should be taken with a grain of salt. Getting a negative result from an antigen test doesn’t give you the green light to behave as though you’re uninfected. The most reliable way to tell if you have Covid or not is to get a PCR test, which is considered the gold standard.[8]
Whether or not Health Canada will approve this new test is not known at this time. They are currently considering numerous applications for such quick response at-home tests. What we do know is that they have refused approval for similar at-home antigen tests in the past:
Where are Canada’s rapid at-home coronavirus tests? Infectious disease experts have been asking themselves — and public health officials — this for months. “If every Canadian had that in their medicine cabinet, we might be able to test our way out of this,” said Colin Furness, an infection control epidemiologist and assistant professor at the University of Toronto… …Furness is hopeful for a wider approval. He said at-home tests have the ability to not only assist busy public health agencies but also help keep businesses and schools afloat.[9] “We have to think of it like a screening tool, a magic thermometer,” he said. “It doesn’t provide you a diagnosis but it tells you something’s wrong.”[10]
Other medical experts are collectively shaking their heads at the poor policies in place for the approval and massive distribution of such at-home rapid-testing kits.
Many of these tests have gotten a “bad rap” because they’re considered less sensitive than lab-based tests, said Dr. Prabhat Jha, an epidemiologist at the University of Toronto, and director of the Centre for Global Health Research at St. Michael’s Hospital…Jha believes there’s too much weight being put on this threshold. He believes an effective home testing strategy is a critical part of Canada’s response to the second wave of the virus.[11]
Based on this information, are we safe to infer that if we had such tests back during the summer, we could have drastically reduced the number of infections that led to the second wave?
“Making them available to nursing home staff, for example, would be worth it. Sure, there’d be some you miss, but you could substantially reduce the number of people who are showing up positive at a nursing home, asymptomatically,” he said. “We don’t have to let the perfect be the enemy of the possible.” [12]
It seems as though we have been waiting a long time for such tests. I never imagined that, during a global pandemic, several vaccinations would be discovered and widely distributed before a single, reliable, rapid-response at-home test could be produced.
Isolation:
At this point in time – mid to late December, 2020 – we find ourselves in Canada faced with a rapidly rising second wave of infections. Many restrictions have been placed across the country. We are seeing a rate of 2400 cases a day in Ontario. This is four times higher than during the first wave in March-April. For various reasons – people ignoring social restrictions, businesses staying open, lax enforcement of Covid-19 regulations, kids returning to school, pandemic fatigue, excitement for a vaccine, etc. – the rate of infections has steadily increased since the end of the summer. Governments are forced to impose tougher restrictions on ‘hot spots’ which, in turn, causes residents of that area to move into less restricted areas to shop, dine, etc., which eventually causes a greater spread of infections turning that area into a ‘hot spot’ and so on, and so on, ad nauseum.
It is discouraging to see how some absolutely ridiculous policies were put in place regarding isolation with Covid-19. From the Ontario Provincial Ministry of Health’s website, the following protocol can be found on the ‘COVID-19 Screening tool for students and children in school and child care’ (Version 3: October 5, 2020): “Household members without symptoms may go to school/child care/work.”[13] Think about this for a second. What’s wrong with this statement? Quite a bit, actually. First of all, it commits the fallacy of ‘begging the question’ by assuming that only those people showing signs of the virus are a threat and need to stay home. However, as we all have known for a very long time, it is those who are asymptomatic who are the greatest spreaders of the virus. In fact, the latest research indicates that those who are asymptomatic far outnumber those who are not by a ratio of up to 3 to 1.[14] Because of this policy, thousands upon thousands of unsuspecting and asymptomatic people – especially elementary school-aged children – will attend school to spread the disease to other unsuspecting children who show no signs of the illness but who will quite likely pass it on to their unsuspecting older siblings, parents, and grandparents. In effect, this policy allows for an extremely effective way of transmitting the virus throughout a given population. Such a policy has allowed very young children to become central vectors in transmitting the disease. It is a self-defeating, ill-conceived policy, and it needs to stop – immediately! I have been trying to relay this to the Minister of Education, Stephen Lecce, and the Premier of Ontario, Doug Ford, for months; but to no avail.
Any and all such policies which assume – falsely – that checking for Covid symptoms amounts to preventing the spread of the virus, are flawed. So any person who is asymptomatic can leave a household entirely infected with Covid-19 and return to work, or attend school, or go to a daycare. A more comprehensive policy might have included something akin to the following protocol: Whenever any person within a household is positively diagnosed with Covid-19, ALL members of that household should remain isolated. When – AND ONLY WHEN – every person in that household produces a negative test result from a PCR testing site, should they end their isolation. By allowing all non-symptomatic members of an infected household to move throughout the community governments have initiated a policy which has rapidly increased the rate of spread of infection.
What we might want to consider at this point is: Who created this part of the policy for isolation regarding Covid-19? Was it a single person? A committee? How were medical professionals consulted on such a development? Citizens have a right to know; because this small technicality may be largely responsible for the rapid transmission of the virus throughout Ontario.
There are other problems involving isolation – or perhaps, more accurately – non-isolation. ‘Anti-maskers’ are people who believe that wearing a mask while in public places, is unnecessary. They sometimes hold large anti-lockdown freedom marches. Not unlike Trump rallies, such events are both highly politicized and often become super spreader gatherings. Wearing a mask is no longer seen as a public duty i.e. “We’re all in this together”. Instead, wearing a mask is viewed as a symbol of political oppression i.e. “No way, is ‘the man’ or ‘Big Government’ going to tell me what to do!” There are many factions of society – from Mennonite communities, to New Age devotees, to far-right conservatives – who show up for such marches.
It is science which has led the way throughout this entire pandemic.
There is a general feeling of anti-science in the air. And that is unfortunate; for it is science which has led the way throughout this entire pandemic.[15] From our decades-long predictions and warnings, to pleading for attention that this pandemic was inevitable, to the understanding of its cause, to its genetic identification, vaccination development, etc., science has been at the forefront leading and advising us of the most responsible actions to take. In world-record-breaking time, several vaccinations have been produced to put an end to the virus so the world can return to some form of normalcy. To see such people flout the value of scientific evidence because of their oddly-kept and deeply skewed views of liberty and freedom has such ironic flavour as to go entirely unnoticed beneath their watch. Anti-maskers are wrong. Period. Wear a mask; it’s among the very least you can and hence, should do – for your community, your country, your world. Science proves that masks work; therefore, you listen to science and wear a mask – irrespective of any and all political ideologies.[16]
Anti-Virals:
The biggest news to date with antivirals is that the Latest COVID-19 guidelines have come out against two leading antivirals: bamlanivimab and remdesivir. In a recent paper, it was found that:
…there are insufficient data to recommend either for or against the use of bamlanivimab for the treatment of outpatients with mild to moderate COVID-19. The drug should not be considered the standard of care, and hospitalized patients should not receive bamlanivimab outside of a clinical trial, according to the treatment panel. It recommended that clinicians discuss trial participation with patients and prioritize use of the drug in patients with the highest risk of COVID-19 disease progression.[17]
Dexamethasone and convalescent plasma treatments continue to be used successfully in ICU’s throughout the world.
Vaccines:
There has been considerable development of vaccination therapies since Part III of this series. As of mid-December, 2020 the world is now receiving vaccinations from two major companies: Pfizer and Moderna. Both are mRNA vaccines which is a very new form of technology which was developed in accordance to discoveries made by 2020 Nobel Prize Laureates Drs. Emmanuelle Charpentier and Jennifer A. Doudna.
That method, formally known as CRISPR-Cas9 gene editing but often called simply CRISPR, allows scientists to precisely cut any strand of DNA they wish. In the 8 years since its creation, CRISPR has been a boon for biologists, who have published thousands of studies showing that the tool can alter DNA in organisms across the tree of life, including butterflies, mushrooms, tomatoes, and even humans.[18]
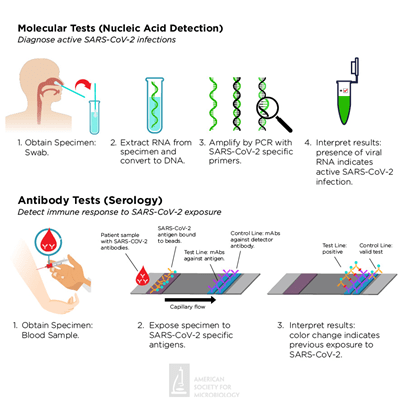
This same technology has allowed scientists to rapidly develop vaccines against Covid-19. Known as mRNA (or messenger ribonucleic acid):
COVID-19 mRNA vaccines give instructions for our cells to make a harmless piece of what is called the “spike protein.” The spike protein is found on the surface of the virus that causes COVID-19. COVID-19 mRNA vaccines are given in the upper arm muscle. Once the instructions (mRNA) are inside the immune cells, the cells use them to make the protein piece. After the protein piece is made, the cell breaks down the instructions and gets rid of them. Next, the cell displays the protein piece on its surface. Our immune systems recognize that the protein doesn’t belong there and begin building an immune response and making antibodies, like what happens in natural infection against COVID-19. At the end of the process, our bodies have learned how to protect against future infection. The benefit of mRNA vaccines, like all vaccines, is those vaccinated gain this protection without ever having to risk the serious consequences of getting sick with COVID-19.[19]
Currently, both the Pfizer and Moderna vaccines are being shipped to enormous freezers which must keep them at very cold temperatures: Pfizer at -75o C and Moderna at – 20o C.[20] This will obviously complicate logistics. But many countries have already established guidelines and supply chain management strategies in an effort to optimize deliveries of the vaccine.
Triage: Who Gets the Vaccine First?
Since this is our first pandemic, determining the triage or order of preference for a medical intervention is a political, legal, and moral determination. In regards to which countries first receive the vaccine, Canada is involved with a coalition known as COVAX:
COVAX is a global initiative led by the WHO, the Coalition for Epidemic Preparedness Innovations (CEPI) and international vaccine alliance organization Gavi, that aims to bring governments and vaccine manufacturers together to ensure all countries have access to the COVID-19 vaccine once they become available.[21]
So far, there are approximately 184 countries participating in the COVAX program. But this does not limit wealthier nations (like Canada) from reaching out directly to pharmaceutical companies in procuring vaccines:
Higher-income countries are not limited to resorting to COVAX just because they’ve signed on. Several, like Canada and the European Union, have been dealing directly with pharmaceutical companies to secure vaccine doses. To date, Canada has procured nearly 414 million vaccine doses — more than 10 doses per-person for its population of 37.9 million while the European Union, which is home to almost 448 million people, is also on track to obtain 1.1 billion COVID-19 vaccine doses. In a statement to Global News, the office of the Prime Minister said that Canada had announced $440 million into COVAX — the second largest contribution any country has made so far.[22]
So, as a country, Canada seems well-positioned in receiving various vaccines as they become approved for world-wide distribution. In regards to who, exactly, will be receiving the vaccines as they arrive, we notice that a system of priorities has been put in place. On the Government of Canada’s website, we find the following guidelines:
The objective of this advisory committee statement is to provide preliminary guidance for public health program level decision-making to plan for the efficient, effective, and equitable allocation of a novel coronavirus disease 2019 (COVID-19) vaccine once it is authorized for use in Canada when limited initial vaccine supply will necessitate the prioritization of immunization in some populations earlier than others. These recommendations aim to achieve Canada’s pandemic response goal: “To minimize serious illness and overall deaths while minimizing societal disruption as a result of the COVID-19 pandemic.” Due to anticipated constraints in supply, these National Advisory Committee on Immunization (NACI) recommendations apply to provincial/territorial publicly-funded immunization programs only and not for individuals wishing to prevent COVID-19 with vaccines not included in such programs.[23]
There are specific key populations that have been identified as priority status. Such key populations include at high risk of severe illness and/or death from COVID-19 includes:
Advanced age, those most likely to transmit COVID-19 to those at high risk of severe illness and death from COVID-19 and workers essential to maintaining the COVID-19 response, Healthcare workers, personal care workers, and caregivers providing care in long-term care facilities, or other congregate care facilities for seniors, other workers most essential in managing the COVID-19 response or providing frontline care for COVID-19 patients, household contacts of those at high-risk of severe illness and death from COVID-19, those contributing to the maintenance of other essential services for the functioning of society, those whose living or working conditions put them at elevated risk of infection and where infection could have disproportionate consequences, including Indigenous communities.[24]
The following graph summarizes the National Advisory Committee on Immunization’s (or NACI) interim recommendations on key populations for early COVID-19 immunization for public health program level decision-making:

Good News…bad news.
So the good news is: the end to the pandemic is in sight. The bad news is that by the time vaccinations get into the arms of enough Canadians to reach actual herd immunity (70+%), many will become sick and many more will continue to die. We have learned, recently, that such a tactic of deliberately allowing millions to become infected with the virus to quicken the likelihood of herd immunity was carried out by the Trump Administration:
A top Trump appointee repeatedly urged top health officials to adopt a “herd immunity” approach to Covid-19 and allow millions of Americans to be infected by the virus, according to internal emails obtained by the House Oversight Committee and shared with POLITICO. “There is no other way, we need to establish herd, and it only comes about allowing the non-high risk groups expose themselves to the virus. PERIOD,” then-science adviser Paul Alexander wrote on July 4 to his boss, Health and Human Services assistant secretary for public affairs Michael Caputo, and six other senior officials.[25]
At first sight, one might think this might be an effective way to try to battle a virus. However, upon further consideration, it becomes quickly apparent that far more people will fall ill and die as a result. For example, if just 1% of those infected with Covid-19 die, and 300 million Americans contract it in an effort to hasten herd immunity, then that means around 3 million people in the US, alone, will die. Trump’s appointee furthers his illogical suggestion by saying:
“Infants, kids, teens, young people, young adults, middle aged with no conditions etc. have zero to little risk….so we use them to develop herd…we want them infected…” Alexander added. “[I]t may be that it will be best if we open up and flood the zone and let the kids and young folk get infected” in order to get “natural immunity…natural exposure,” Alexander wrote on July 24 to Food and Drug Administration Commissioner Stephen Hahn, Caputo and eight other senior officials.[26]
Here’s where things get interesting and perhaps, a little frightening. If, and I say: IF, Paul Alexander was aware of the projected death rate, and he continued to push for his bizarre idea of bringing about herd immunity, THEN it follows that he was willing to sacrifice a great many lives in order to speed up the movement of the virus through the US population – and the number of lives sacrificed would be well into the millions. What’s more, the suggestion of such an idea makes a great deal of sense now that we recall how states like Florida and Texas simply ignored CDC and WHO guidelines for dealing with the virus and let all businesses stay open and resume as usual. And perhaps this is why Trump was downplaying the use of masks and holding such enormous rallies:
Alexander also argued that colleges should stay open to allow Covid-19 infections to spread, lamenting in a July 27 email to Centers for Disease Control Director Robert Redfield that “we essentially took off the battlefield the most potent weapon we had…younger healthy people, children, teens, young people who we needed to fastly [sic] infect themselves, spread it around, develop immunity, and help stop the spread.”[27]
There is no definitive evidence that Alexander’s suggestions were fashioned into any type of formal policy: “In a statement, a Health and Human Services spokesperson said that Alexander’s demands for herd immunity “absolutely did not” shape department strategy.”[28] Be that as it may, to what extent did such an idea lie in the backs of the minds of those who neglected to act quickly and decisively against the spread of such a deadly virus? Especially when another main chief medical advisor to President Trump, Dr. Scott Atlas, was a major advocate in promoting herd immunity:
During a Fox News appearance on Aug. 3 discussing college reopenings, Atlas echoed an argument often made by Trump that children “have no risk for serious illness” and “they’re not significant spreaders,” adding, “There should never be and there is no goal to stop college students from getting an infection they have no problem with.”[29]
Practically all public health care professionals have argued the opposite and have now recognized the crucial role people who are asymptomatic play in transmitting and spreading the disease:
While researchers are still studying the effects of the virus on children, a study published in JAMA Pediatrics in July found children carry as much or more of the infection in their noses and throats compared to adults, while a Centers for Disease Control and Prevention contact tracing study found young people between ages 10 and 19 years old are more likely to spread the coronavirus in households, where other family members may be more susceptible to severe symptoms.[30]
Donald Trump has surrounded himself with ‘yes men’ for his entire Presidency. For those who dare to question, they have been shown the door and ridiculed on Twitter. To know just how bad Dr. Atlas’s advice has been, we need look no further than an endorsement from the President himself:
“Scott is a very famous man who’s also very highly respected,” Trump said on Monday. “He’s working with us and will be working with us on the coronavirus,” Trump said in August. “And he has many great ideas. And he thinks what we’ve done is really good, and now we’ll take it to a new level.”[31]
Notice how Trump refers to Atlas’s apparent ‘fame’ first? Trump has always cared more about vacuous and value-starved credentials like ‘fame’ and ‘ratings’ as sign-posts for excellence in his concept of professionalism rather than virtues like honesty, integrity, earned professional merit, and dependability. For anyone to think that the Trump Presidency’s task force on Covid-19 (led by Vice President Mike Pence) was “really good”, demonstrates a blind obedience to a political power and indicates a person who has surrendered the values of science as being impartial and objective.
Before joining Trump’s Covid-19 ‘Task Force’, Atlas held a position as senior fellow at Stanford University’s Hoover Institution, a conservative think tank. Atlas himself is not an infectious disease expert but a board-certified diagnostic neuroradiologist and has served as a professor and chief of neuroradiology at Stanford University Medical Center from 1998 to 2012. His highly-politicized medical advice regarding the pandemic has been met with swift and fierce rebuke from his colleagues at Stanford. In a scathing letter, dozens of Stanford University Medical School’s top faculty denounced their former colleague for promoting what they called “falsehoods and misrepresentations of science”:
“Many of his opinions and statements run counter to established science and, by doing so, undermine public-health authorities and the credible science that guides effective public health policy,” according to the letter, signed by Dr. Philip A. Pizzo, former dean of Stanford School of Medicine; Dr. Upi Singh, chief of Stanford’s Division of Infectious Diseases, and Dr. Bonnie Maldonado, professor of epidemiology and population health, and 105 others.[32]
When scientific knowledge loses its objectivity and professionals decide to weaponize such misleading information, people suffer, and people die. And this is exactly what we have been seeing because of extremely poor leadership on the part of Mr. Trump, and unforgiveable behaviour on the part of Dr. Atlas. In my estimation, ‘Dr.’ Atlas should have his medical degree suspended or stripped for spreading such medical misinformation. We shall see if any professional repercussions ensue in the following months.
The importance of why world leaders must be well-informed and guided by professional advisers who provide the most current and accurate scientific information cannot be overstated. To ignore this, is to do so at the peril of many innocent people.
We did not meet the second wave with the same amount of dedication as we did with the first wave. And unfortunately, this is showing in the number of cases, hospitalizations, and deaths throughout the world. Hopefully, we will be able to flatten the curve on this wave as quickly as possible so we are all in a much better position to reach peak immunization when the vaccine becomes available to us.
NOTE: I am not going to waste any time discussing the anti-vaccination position. The bottom line is this: Anti-vaxxers are wrong. If the Covid-19 vaccination poses no real health threat to you, it automatically becomes your prima facie minimal duty – to yourself, to others, to your country, and to the world, to get it.
Dealing with Anxiety by Battling Misinformation
Emotionally, the pandemic has taken its toll on us. It is difficult to say at this point, how long after the world returns to normal will we need to deal with issues of anxiety and PTSD. As many are facing pandemic fatigue and are simply tired of having their lives affected by such a pathogen, we must remain vigilant in following rigorous protocols of physical distancing, mask-wearing, handwashing, testing, tracking and tracing, and patience in waiting for our turn to get the vaccine. We can best deal with anxiety when we start with solid, reliable, and responsibly-attained information. If anyone reading this series of papers has any questions regarding the scientific soundness of available information, there are plenty of websites available to help:
https://en.ccunesco.ca/blog/2020/10/fighting-disinformation-during-a-pandemic
https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/fighting-disinformation_en
https://www.nature.com/articles/d41586-020-01834-3
If you are unable to find answers to your questions regarding reliable information about Covid-19, feel free to reach out to me, personally and I will do my best to comply. I can be reached at: cdicarlo@criticalthinkingsolutions.ca.
Conclusion:
We will get through this. And we will all be the better for it. For it is in such times of crises that we discover the value and the virtue of the human condition. Here’s hoping that my next paper will report incredible progress against this virus not only in Canada, but throughout the rest of the world. And may it also be the last paper I will need to write about Covid-19.
[1] https://academic.oup.com/jxb/article/60/3/712/453685
[2] See: https://www.dovepress.com/three-quarters-of-people-with-sars-cov-2-infection-are-asymptomatic-an-peer-reviewed-article-CLEP
[3] https://www.dailymail.co.uk/news/article-9058923/New-Covid-strain-17-mutations-scientist-say.html?ito=push-notification&ci=60538&si=17097303
[4] Ibid.
[5] https://www.nytimes.com/2020/11/27/science/covid-vaccine-virus-resistance.html
[6] Ibid.
[7] https://www.cnbc.com/2020/12/16/fda-approves-ellume-home-covid-test-how-it-works-and-antigen-accuracy.html
[8] Ibid.
[9] https://globalnews.ca/news/7469571/coronavirus-canada-rapid-at-home-tests/
[10] https://globalnews.ca/news/7469571/coronavirus-canada-rapid-at-home-tests/
[11] Ibid.
[12] Ibid.
[13] https://covid-19.ontario.ca/covid19-cms-assets/2020-10/Printable%20school%20and%20child%20care%20screening_v3_en.pdf
[14] See: Peterson, I., and Phillips, A. (2020). Three-Quarters of People with SARS-CoV-2 Infection are Asymptomatic: Analysis of English Household Survey Data. Clinical Epidemiology. https://www.dovepress.com/three-quarters-of-people-with-sars-cov-2-infection-are-asymptomatic-an-peer-reviewed-article-CLEP
[15] See: https://www.theatlantic.com/magazine/archive/2021/01/science-covid-19-manhattan-project/617262/
[16] Obviously, this excludes health-based and all other relevant reasons for not being able to wear a mask.
[17] https://acpinternist.org/weekly/archives/2020/11/24/1.htm
[18] https://cen.acs.org/biological-chemistry/gene-editing/CRISPR-genome-editing-2020-Nobel/98/i39#:~:text=The%202020%20Nobel%20Prize%20in,strand%20of%20DNA%20they%20wish.
[19] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html
See also: https://www.nature.com/articles/nrd.2017.243
[20] There are also the Oxford-AstraZeneca and the Johnson & Johnson vaccines which are expected to receive approval for widespread distribution soon.
[21] https://www.msn.com/en-ca/news/world/your-guide-to-covax-the-whos-coronavirus-global-vaccine-plan/ar-BB1bwZZK?ocid=iehp&li=AAggNb9
[22] https://www.msn.com/en-ca/news/world/your-guide-to-covax-the-whos-coronavirus-global-vaccine-plan/ar-BB1bwZZK?ocid=iehp&li=AAggNb9
[23] https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/guidance-key-populations-early-covid-19-immunization.html
[24] https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/guidance-key-populations-early-covid-19-immunization.html
[25] https://www.msn.com/en-ca/news/newspolitics/we-want-them-infected-trump-appointee-demanded-herd-immunity-strategy-emails-reveal/ar-BB1bZ5h3?ocid=iehp&li=AAggNb9
[26] Ibid.
[27] Ibid.
[28] Ibid.
[29] https://www.forbes.com/sites/mattperez/2020/08/12/who-is-dr-scott-atlas-trumps-new-covid-health-adviser-seen-as-counter-to-fauci-and-birx/?sh=6336011720a4
[30] Ibid.
[31] https://www.cnn.com/2020/11/16/politics/atlas-stanford-coronavirus-michigan/index.html
[32] https://www.mercurynews.com/2020/09/12/stanford-doctors-take-aim-at-former-colleague-scott-atlas-trumps-new-adviser-on-the-covid-19-pandemic/
The views, opinions and analyses expressed in the articles on Humanist Freedoms are those of the contributor(s) and do not necessarily reflect the views or opinions of the publishers.
Featured Photo Courtesy of: https://www.baystatehealth.org/covid19









:focal(373x167:374x168)/https://public-media.si-cdn.com/filer/6f/ab/6fab9422-3d12-45b0-b9e2-38bc667561a5/ppeportrait1.jpg)